ArcheMedX Releases Largest Confidence-Based Assessment Dataset in CNS Clinical Research at CNS Summit 2025
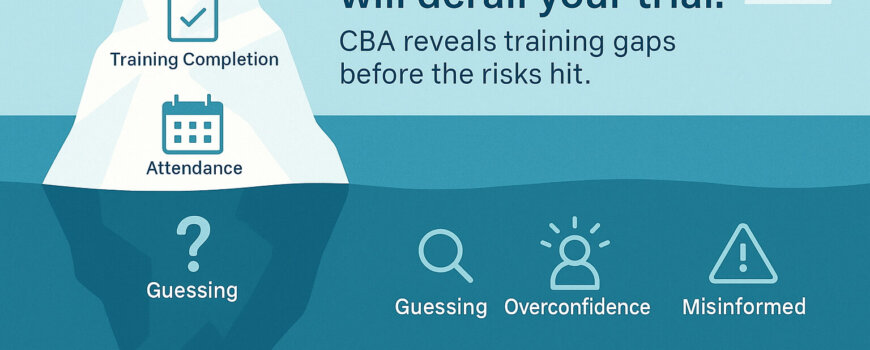
ArcheMedX shares the largest CBA dataset in CNS trials, revealing hidden training risks and how to reduce them

ArcheMedX shares the largest CBA dataset in CNS trials, revealing hidden training risks and how to reduce them

The compounding benefits of effective training cannot be overstated. When clinical research associates (CRAs) and site staff are thoroughly prepared, they engage more deeply with the trial protocols, ask more insightful questions, and more proactively anticipate challenges.
The formal Formal adoption of the E6(R3) guideline introduces a proportionate and more modern risk-based approach to quality management. Clinical trial leaders must implement more effective training programs that address increased trial complexity and ensure compliance with the enhanced quality requirements.

Ready has powered more than 1,000,000 user sessions with clinical professionals from over 90 countries to become the preferred study training tool for over 80% of site personnel.

Trial leaders recognize traditional site initiation processes often lead to excessive delays but have struggled to adapt and improve.
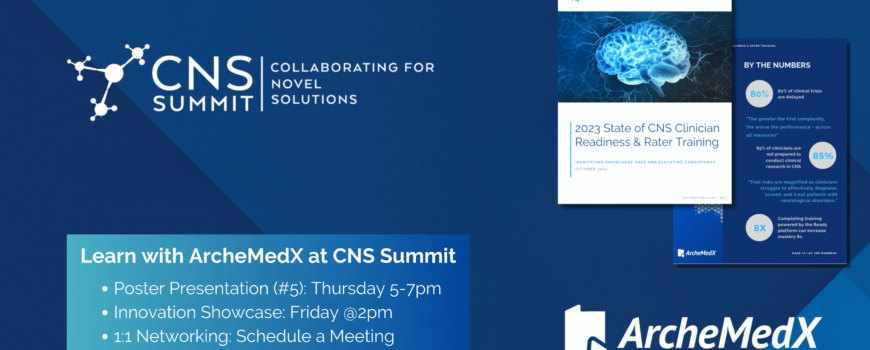
Analyses of 95,724 clinician learners across CNS-related conditions demonstrated significant knowledge gaps and increases in clinical mastery, learn more with ArcheMedX at the CNS Summit

Explore how behavioral science can revolutionize clinical trial methodologies and overcome operational challenges. Dive deep into the interplay between human behavior and clinical research with insights from Dr. Brian McGowan and the ArcheMedX team.

54,000 Healthcare Providers dramatically increased their knowledge and confidence in effectively diagnosing, treating, and managing patients with pain after completing more interactive medical education powered by ArcheMedX

How can you minimize the performance risks given the complexities of a clinical trial and be ready to effectively conduct your next study?
We found that employees with a more incremental mindset have higher job performance.